- New Prescriptions
- Rx Processing Alerts
- Verification
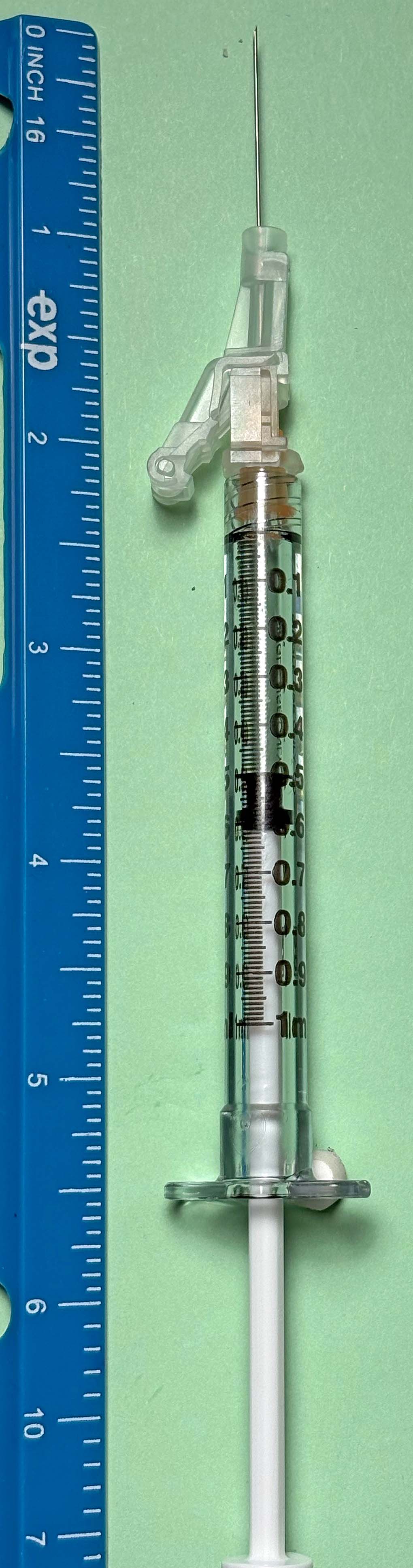
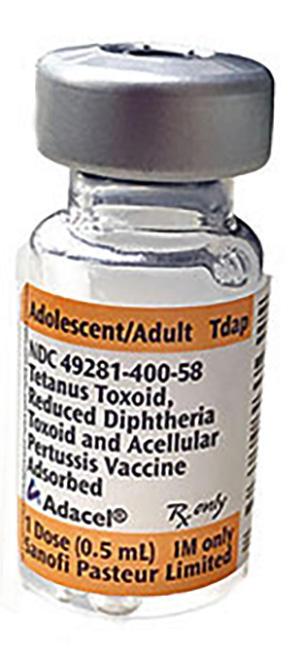
- Dispensing
- RX Counseling
- OTC Counseling
- Clinical Services
- Drug Info
- Other Functions
 |
| Pharmacist Verification | |||
| Select Pharmacist Action: | |||
| Click the Buttons to View | |||
Patient Consent Form
| 1. Patient Information | |||
|---|---|---|---|
| 2. Insurance Information | |||
|---|---|---|---|
| 3. Screening Questions | Yes / No | |
|---|---|---|
| Are you currently sick or experiencing a high fever today? | ||
| Do you have severe allergies to medications, foods (e.g., eggs), or latex? | ||
| Have you ever had a serious reaction to a previous vaccine, including dizziness/fainting? | ||
| Do you have a bleeding disorder or are you taking blood thinners? | ||
| Are you immunocompromised (e.g., cancer, HIV, steroid medications)? | ||
| For women: Are you currently pregnant or breastfeeding? | ||
| 4. Consent & Signature | |
|---|---|
|
I have read the information regarding the vaccine. I have had the opportunity to ask questions that were answered to my satisfaction. I believe I understand the benefits and risks of the vaccine and ask that the vaccine be given to me or to the person named above for whom I am authorized to make this request. |
|
| Robert Elder | |
| 5. For Office Use Only | |||
|---|---|---|---|
 |